

What’s Working—and What Needs Fixing—in Lesotho’s Cervical Cancer Vaccine Programme
5 May 2026 by Pascalinah Kabi

A pile of yellow booklets, decorated with animated visuals of family members—children, mothers, and health symbols—sits on a brown desk at Boitelo English Medium School in Mafeteng District.
Two nurses and a village health worker flip through the booklets, searching for girls aged 9–14 who have not received the vaccine that prevents one of the most dangerous non-communicable diseases—cervical cancer.
They are looking for these girls as Lesotho Ministry of Health intensifies its campaign to eliminate cervical cancer by 2030, in line with the 2020 global targets set by the World Health Organisation.
According to these targets, countries must meet the 90–70–90 benchmarks by 2030:
- 90 percent of girls fully vaccinated with the HPV vaccine by age 15
- 70 percent of women screened with a high-performance test by ages 35 and again by 45
- 90 percent of women identified with cervical disease receiving treatment (including 90 percent of those with pre-cancer and 90 percent of those with invasive cancer).
From rapid gains to sudden decline
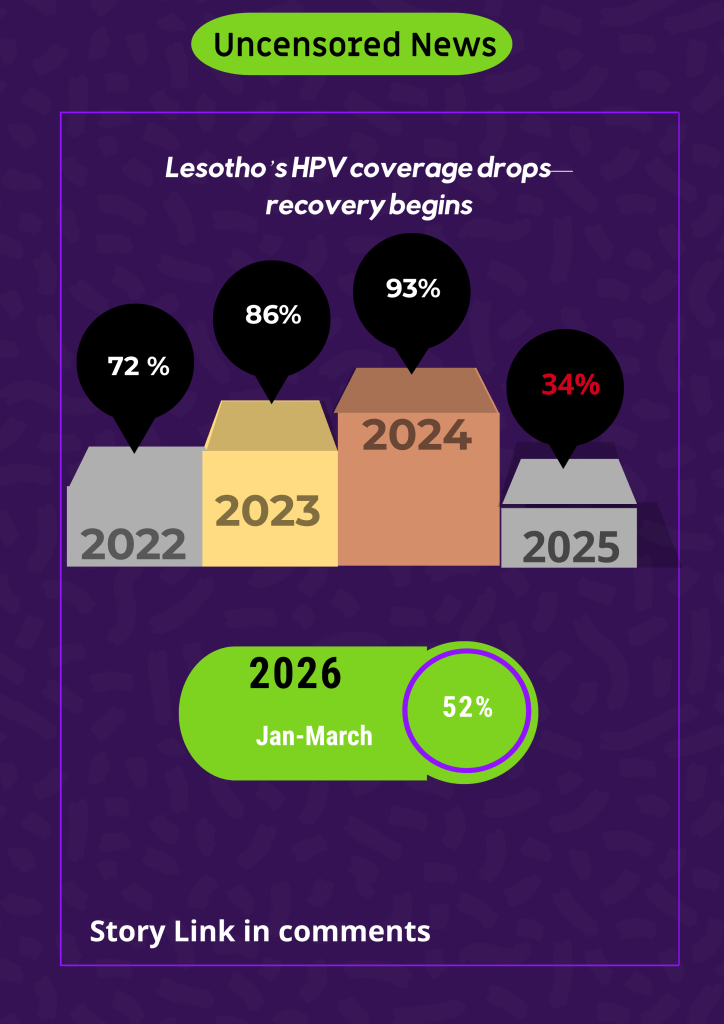
When the country launched a large-scale HPV vaccination campaign in 2022, it recorded a 72 percent national coverage rate, with Botha-Bothe achieving the highest coverage at 98 percent, while Thaba-Tseka lagged at 59 percent. In 2023, coverage increased steadily to 86 percent, with Mafeteng and Botha-Bothe both reaching 99 percent, with Maseru recording the lowest coverage at 72 percent. The national rate rose further to 93 percent in 2024, with Berea and Botha-Bothe exceeding targets at 103 percent, while Maseru recorded the lowest coverage at 86 percent.
During these three years, the Ministry of Health delivered HPV vaccines to communities through village and school-based outreach programmes, supported financially by Gavi, the Vaccine Alliance.
However, a shift to integrating the HPV vaccine into routine immunisation led to a sharp decline in coverage—from steady gains to a national rate of just 34 percent in 2025. Mokhotlong recorded 55 percent coverage, while Maseru vaccinated only 27 percent of its target population of girls aged 9–14.
Between January and March 2026, the country recorded a partial recovery, reaching 52 percent national coverage. Quthing exceeded targets at 167 percent, while Botha-Bothe dropped significantly to just six percent.The Lesotho Ministry of Health says it aims to sustain the 2026 momentum and has introduced school-based outreach registers this year—an approach credited with improving coverage from 34 percent in 2025 to 52 percent in the first three months of 2026.
The Expanded Programme on Immunisation (EPI) has also recruited outreach coordinators in five districts supported by Gavi under the Equity Accelerator Fund. These coordinators are primarily responsible for tracing and linking zero-dose and under-immunised children, as well as HPV-eligible girls to vaccination services.
In addition, Gavi has donated five vehicles to support outreach programmes in the targeted districts. On what will happen in the remaining five districts not covered by Gavi funding, the Ministry of Health said other partners, including UNICEF and the World Health Organisation, are working to ensure those areas also receive outreach support.
A vulnerable promise

Lesotho’s HPV coverage data from 2022 to the first quarter of 2026 shows that the vaccination programme has delivered both “promise and vulnerability.”
Dr Howard Ndaba, a clinical oncologist, told Uncensored News on 4 May 2026 that the HPV vaccination programme continues to reflect both “promise and vulnerability.”
“Data from 2022 to 2024 indicate that the country achieved high vaccination coverage across multiple districts, in some cases approaching or exceeding the World Health Organisation (WHO) target of 90 percent of girls vaccinated by age 15,” Dr Ndaba opened.He added: “This demonstrates strong implementation capacity, effective outreach, and initial public acceptance. It confirms that, operationally, Lesotho is capable of delivering a high-impact cancer prevention programme.”
He however warned that recent data from 2025 to early 2026 reveal a marked decline in vaccination coverage, with many districts dropping to moderate or low levels.
He explained that this shift suggests challenges in sustaining programme performance beyond initial campaigns. “Possible contributors include transition to routine immunisation systems, logistical or supply constraints, and reduced community engagement.”
Critically, Dr Ndaba warned, cervical cancer elimination requires consistent, sustained high coverage, not intermittent success.
“The observed decline therefore indicates that we are not yet firmly on track for elimination, despite a strong foundation. Despite this, we have proven that high coverage is achievable, but the priority now is maintaining it across all future cohorts. Without stability, earlier gains risk being reversed, leaving gaps in population protection.”
Life-time risks
At the beginning of this year, Lesotho Times reported that Senkatana Oncology Clinic recorded 295 cervical cancer cases between 2024 and 2025. Senkatana’s Nursing Officer, Matselane Motsie, told the publication that 161 cases were recorded in 2024 alone, while 134 Basotho women were diagnosed with this vaccine-preventable disease in 2025.
Dr Ndaba offers a practical, cost-free solution on how Lesotho can eliminate cervical cancer. “HPV vaccination is a direct cancer prevention intervention,” he said.
He warned that persistent infection with high-risk HPV types is the primary cause of cervical cancer, and that vaccination is most effective when administered before exposure—typically before girls become sexually active in early adolescence.
“The data I shared with you highlights an emerging protection gap: earlier cohorts benefited from high coverage, but recent declines mean that new groups of children may remain unprotected,” he warned.
His message to parents and caregivers a clear call to action. “The implication is immediate and consequential. Delaying vaccination increases the lifetime risk of cervical cancer, a risk that cannot be fully reversed later.”
“Unlike many health decisions, this is a time-sensitive intervention with long-term impact. High vaccination coverage also protects communities by reducing HPV transmission overall; declining uptake weakens this collective protection,” Dr Ndaba concluded.
HPV vaccine is not a license for unsafe sexual behaviour
Nurse Limakatso Radebe spends her days at Le Coop Health Centre in Mafeteng, administering the HPV vaccine to girls aged 9–14. In February, she told Paballo-ea-Bophelo—a community-based organisation that benefited from funding from Gavi to reach children in Mafeteng, Maseru, Berea, Leribe, and Mokhotlong—that administering the HPV vaccine is far cheaper than treating a cancer patient.
In Lesotho, the government pays approximately M250,000 per patient for cancer treatment in Bloemfontein, South Africa. Radebe noted that there are sometimes shortages of medication to treat patients.
“When we transfer them to Bloemfontein in South Africa, there is a long waiting list. While on the waiting list, cancer is not treated. It is very expensive—even pain medication is costly,” she said.
Meanwhile, she cautioned that vaccination does not eliminate the need for responsible sexual behaviour.
“We emphasise that being vaccinated does not mean you will never develop cancer, but the chances are significantly reduced. This means condoms must still be used consistently when girls become sexually active. That is why we provide education before vaccination—we want them to grow into future mothers free from cervical cancer,” Radebe said.
She issued a direct appeal to parents and caregivers.
“Vaccines are the most effective and affordable way to prevent disease. Waiting until there is danger is not advisable. The growing number of women coming for cancer screening shows that cancer is already here—and that people are beginning to understand how serious and painful it is.
“Parents should not come alone for screening while denying their children access to vaccines. Please bring children for vaccination. If there are concerns or questions, come to the health facility and seek clarity.
“We should not have to go to schools to find children. When a child turns nine, they should be brought to the facility for the HPV vaccine. It is available every day—there is no need to wait for a special campaign.”